Technology
Technology in Bite Balance and Occlusion Care
Accurate assessment and management of bite balance require a thoughtful integration of analog precision and digital innovation. Both approaches complement each other, enabling reliable, patient-centered, and evidence-based occlusion care. While digital tools provide detailed data and reproducibility, analog methods offer hands-on insight into functional dynamics-together forming a complete clinical picture.




Analog Technology – The Clinical Foundation
Analog methods form the biological and clinical foundation of occlusion assessment. They allow the clinician to directly observe contact patterns, feel resistance, and interpret bite relationships through tactile and visual feedback. This hands-on approach strengthens clinical judgment and deepens understanding of functional harmony between teeth, muscles, and joints. Key analog instruments include:
- Articulating papers and foils – Identify the location and distribution of occlusal contact areas during closure and movement.
- Shimstock foil – Assesses the presence, intensity, and stability of tooth contacts by evaluating whether contacts hold or release under light force.
- Facebows and articulators – Record maxillomandibular relationships and simulate mandibular movements outside the mouth for detailed functional analysis.
Analog methods are indispensable when digital systems are not available and serve as a reliable baseline for cross-verification of digital findings. They promote the development of tactile sensitivity, occlusal awareness, and real-time decision making during patient assessment.
Together, analog techniques cultivate fundamental clinical skill, while supporting accurate and biologically sound occlusal management.


Digital Technology – Precision with Occlusal Scanners
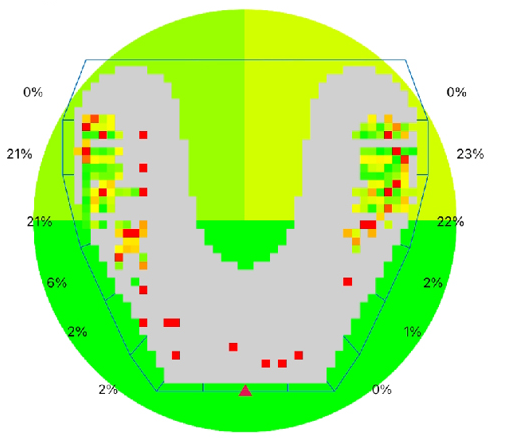
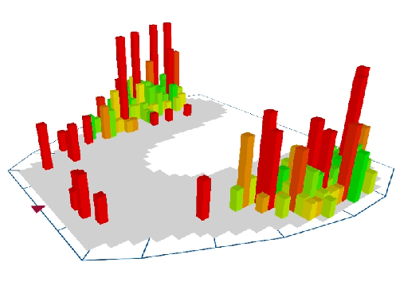
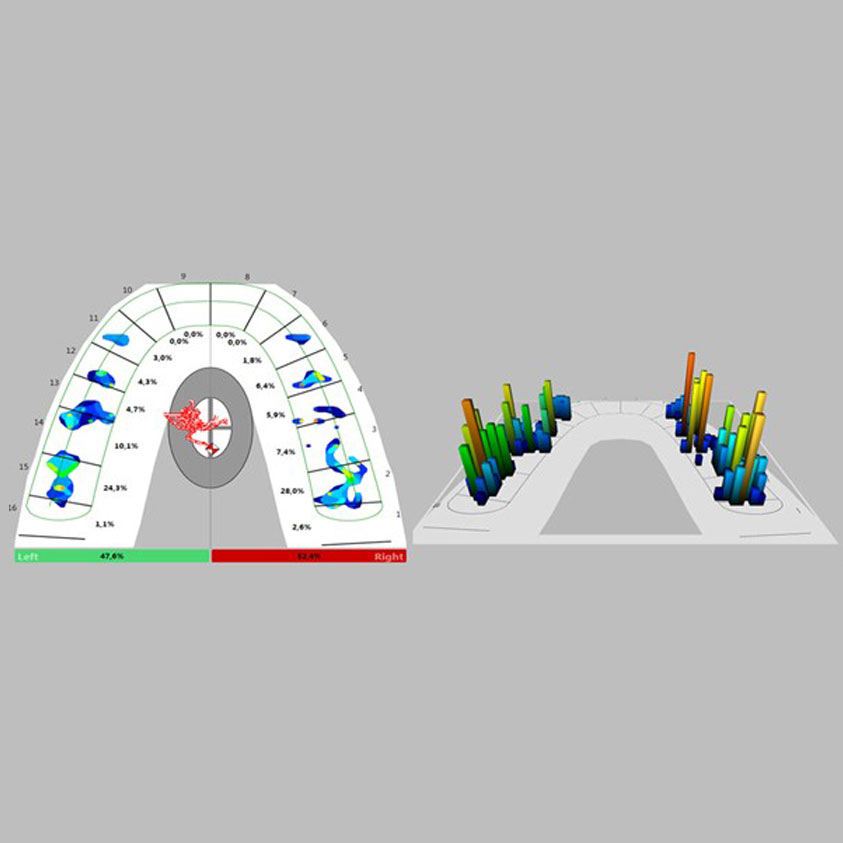
In contemporary occlusion management, digital occlusal analysis systems have significantly enhanced the precision with which clinicians evaluate and manage functional bite disorders. Unlike traditional articulating paper, which merely marks the location of contact points, digital occlusal scanners provide quantitative data on timing, sequence, duration, and relative force distribution of occlusal contacts during mandibular closure and excursive movements.
Occlusion is not a static event; it is a dynamic neuromuscular process. Teeth do not simply “touch” — they interact within an integrated biological system involving the dentition, periodontal ligament mechanoreceptors, masticatory muscles, and temporomandibular joints (TMJs). This coordinated system regulates force magnitude and direction through continuous sensory feedback.
Even minor premature contacts or disproportionate force concentrations can disrupt this functional harmony and may contribute to:
- Masticatory muscle hyperactivity, fatigue, or myofascial pain.
- Tooth sensitivity, microcracks, or cusp fractures.
- Recurrent failure of restorations.
- Excessive loading of dental implants.
- Temporomandibular joint discomfort or dysfunction.
Digital occlusal scanners enable early identification of these functional discrepancies by objectively measuring occlusal force patterns. By detecting abnormal force concentration, prolonged contact timing, or asymmetrical load distribution, clinicians can intervene conservatively and precisely—often before structural damage or symptomatic dysfunction develops.



Adjunct Diagnostic Technologies – Interdisciplinary Bite Assessment
Comprehensive bite assessment extends beyond the identification of occlusal contact points. Occlusion represents a dynamic interaction among teeth, periodontal mechanoreceptors, masticatory muscles, temporomandibular joints, craniofacial skeleton, and airway. Adjunct diagnostic technologies provide structural and functional data that enhance clinical interpretation and support biologically sound decision making.
Occlusal Force Disorders (OFD) are seldom confined to enamel contacts alone. They frequently reflect adaptive or maladaptive responses in bone morphology, condylar position, neuromuscular coordination, disc integrity, and airway dimensions. Advanced imaging and functional tracking systems allow clinicians to visualize and quantify these relationships with greater precision than clinical examination alone.
- Orthopantomogram (OPG) provides a panoramic two dimensional overview of the maxillofacial complex, enabling assessment of dentition, alveolar bone levels, condylar morphology, asymmetry, and gross pathologies that may influence occlusal stability
- Cone Beam Computed Tomography (CBCT) offers three dimensional evaluation of craniofacial structures with high spatial resolution. It permits analysis of condylar position within the glenoid fossa, cortical bone integrity, joint space relationships, implant sites, and airway volume relevant to functional occlusion.
- Magnetic Resonance Imaging (MRI) provides superior soft tissue visualization, particularly of the articular disc, retrodiscal tissues, joint capsule, and associated musculature. It is the imaging modality of choice for assessing disc displacement, inflammatory changes, joint effusion, and internal derangements not detectable with conventional radiography or CBCT.
When integrated with analog examination methods, digital occlusal analysis, and jaw tracking technologies, these adjunct diagnostics create a multidimensional understanding of bite dynamics. They enhance, rather than replace, clinical judgment by correlating structural anatomy with functional performance. This comprehensive approach enables precise, minimally invasive, and biologically guided bite management while preserving the adaptive capacity of the stomatognathic system.